

Mental Health in K12 Is Really Not About the Kids
Mental Health in K12 Is Really Not About the Kids
Schools are injecting mental health interventions into the school day, even though research shows universally applied, “preventative” mental health practices cause harm.


“At conferences, in training seminars, in education schools, [research promoting school-based mental health] is in the air they breathe and water they drink… They then use this research to scare legislatures and governing [education] boards to push a massive, historically unprecedented transformation of U.S. schools into something more akin to health clinics with a classroom attached.”
—
The Centers for Disease Control (CDC) lists a whopping 99 research studies in its document, “Promoting Mental Health and Well-Being in Schools: An Action Guide for School and District Leaders.”



Quite an impressive list, isn’t it?
Or is it?
Researchers in Australia, Chile, and the UK have all come to the same conclusion: Most of the studies on the efficacy of U.S. school-based mental health programs are “unreliable bunk.”
The researchers also have concluded via the gold standard of risk-of-bias analysis that it is highly probable that most studies suggesting universally applied, “preventative” mental health measures in K12 schools produce positive outcomes for kids are manipulated specifically for the purpose of advancing school counseling programs.
Imagine that.
A Legal Process on Substack reports that in 2015, and again in 2021, a team of Australian researchers from the School of Psychology at the University of New South Wales, the National Institute for Mental Health Research, and other institutions, undertook a global, comprehensive systematic review and meta-analysis of research literature examining K-12 school-based counseling intervention programs related to student depression and anxiety.
In total, the Australians put under the microscope 211 English-language, peer-reviewed, randomized control studies involving approximately 47,800 students around the world. 58 of those studies were published in the U.S. involving American school-based behavioral health programs.
A Legal Process reports that the Aussie research team didn’t just compile a survey of studies; they essentially audited all randomized control studies on school-based mental health programs purporting to treat depression and anxiety. And they applied, as ethical meta-analysis researchers do, the international gold standard of risk-of-bias tools to specifically assess the quality of health care research and claims: the Cochrane Review.
In the 2015 systematic review, only 2 out of 27 US-based studies rated "high quality" under the Cochrane Review, leaving a staggering low quality percentage of 92.6%. And only 1 out of the 27 US-based studies at the time could be determined NOT to be selectively reporting data (i.e., containing bias).
In 2021 when they looked again, 84% of the 31 studies were deemed low quality, indicating unreliability and bias, and *zero* of those could be definitively determined NOT to be selectively reporting data.
Both studies found only “very small effects” for actually improving depressive symptoms or anxiety — not just in the U.S., but worldwide.
“Specifically, there are genuine but modest preventive effects of psychological programs delivered at school for depression and anxiety, and the size of the effects dissipate over time.”
Also, to be fair, its not just the U.S studies that are bad:
“Fewer than one-third of all studies [worldwide] were judged as high quality, meaning that most studies involved concerning degrees of risk of bias with significant room for improvement.”
It goes without saying that these findings are tremendously important for anyone seriously concerned with the increasing emphasis in U.S. schools on behavioral and mental health, “wellness,” the popular “Whole Child Whole School” model, “Multi-Tiered Systems of Support” (MTSS), “Community Schools,” School-Based Health Centers (SBHCs), and “Social Emotional Learning” (SEL).
It seems the people working in our schools REALLY want to get into our kids’ heads.
But despite reliable findings by reputable researchers that any positive effects of the above types of things are minimal at best, and not lasting, AND despite evidence that the research data school districts use to justify spending exorbitant amounts of community tax dollars on such things are biased and likely manipulated, the new vocabulary of public education is thoroughly infused with these terms.
A Legal Process writes that this movement didn’t just appear out of the ether: “Professional educators, as a class, being the type of people that won’t express an opinion on a ham sandwich until they’ve read a study validating it, have convinced themselves that schools are not just for the ABCs, but must go beyond boring, run-of-the-mill core academic subjects into comprehensive, mental health services.”
Whole “frameworks” of these things are everywhere in schools.
They have study after study telling them school-based mental health is necessary — and life saving. Even if your local administrator can’t rattle off academic citations, a good many others can and do: “At conferences, in training seminars, in education schools, it is in the air they breathe and water they drink. They then use this research to scare legislatures and governing boards to push a massive, historically unprecedented transformation of U.S. schools into something more akin to health clinics with a classroom attached.”
A team of UK researchers confirmed there is “insufficient evidence" that school-based behavioral health services are effective. They also found that 85% of all studies on the efficacy of these programs are unreliable for bias, writing, “Our findings contradict previously published reviews, as we observed little evidence to suggest that school-based interventions are effective for prevention of anxiety or depression.”
Despite all of these findings, the concerted effort to insert mental health programming into U.S. K12 schools is charging full steam ahead.
A few headlines:
From the article:
And:
The article states that Ohio has more school-based mental health resources than it did seven years ago, and the number of partnerships between community behavioral health centers and schools has more than doubled since 2017. In addition, Ohio has pushed for more on-site care options. In the past two years, Governor Mike Dewine has announced tens of millions of dollars in funding to create or expand school health care centers, which bring a variety of health care professionals into schools.
And:

Here’s video from the article:
And:

The article claims schools can address student absenteeism and other problems by providing school-based mental health services, which could include one-on-one counseling or therapy, case managers who can coordinate various services for students in need, and referrals to outside resources.
In a rare display of common sense, the article suggests schools can address worsening child mental health and academic outcomes by commissioning researchers who can seek to better understand the underlying causes of increasing mental health concerns and absenteeism in children. (Because half of solving a problem is actually identifying the problem.)
Interestingly, the article also suggests, “Research is also needed to explore differences in the relationship between mental health and school outcomes for different subgroups of students – by income level or by racial subgroups. This can potentially inform how schools to respond to problems that threaten student well-being.”
And:
From the article:
And:

The article quotes Pennsylvania Governor Shapiro:

And wouldn’t you know it? We’re still not doing enough:

The article explains how the CDC has released the results of its biennial Youth Risk Behavior Survey earlier this month, highlighting changes in students’ responses from 2021 compared to 2023.
Over those two years, the percentage of students overall who reported feeling persistent sadness fell slightly (by 2 percent). Separated by gender, the percentage of girls reporting feeling hopeless and who said they considered suicide in the previous year both decreased.
In 2023, Hispanic students reported lower rates of persistent sadness, overall poor mental health, thoughts of suicide and planning suicide. The rate of Black students attempting and being injured during suicide attempts both declined.
The article continues: While those recent improvements are heartening, the report also shows that mental health and well-being trends over the past 10 years are mostly heading in the wrong direction. The 2023 data reveals that students are reporting skipping school more frequently due to safety concerns and experiencing more bullying, both of which increased by 4 percent since 2021.
Erica Fener Sitkoff, senior vice president of mental health strategy at FullBloom, a company that provides behavioral health programs for schools, says the findings of the Youth Risk Behavior Survey mirrors what her organization sees in the schools where it helps develop mental health support for students:
“[It] tells us that positive change is possible, and the improvements are encouraging,” she says. “That tells us that the increased awareness and unprecedented funding that’s come since the pandemic are working. It also tells us one year of reversing the trend doesn't mean we can let up, because the numbers still aren’t great. We should dig deeper and invest more in what’s working.”
Fener Sitkoff says schools need to get students mental health support before they reach a crisis, while also preserving the bandwidth of counseling staff. She says schools can strengthen their mental health scaffolding through the addition of what she calls universal skills curriculum, despite the fact that research shows broad, universally applied mental health practices in schools actually worsen kids’ mental health.
And:
Can you predict what the answer will be? I bet you can. Here’s the story.
From the article:

And:
This is in California. Here’s the story.
And:
And:
This is in Michigan. Here’s the story.
The article reports that student mental health was the focus at a recent State Board of Education meeting, where state officials heard from educators on efforts to support children across Michigan.
“When students have access to mental health supports at school, they are six times more likely to receive the interventions they need so they can be the best students possible,” said Diane Golzynski, deputy superintendent of the Michigan Department of Education.
So, if schools have mental health services on site, kids are more likely to receive interventions. Logical.
I wonder where she got the statistic?
According to the article, Michigan teachers say they’ve been updating their practices with changes in technology, using online services to streamline the process for students to receive mental health care.
Since 2020, over 1,000 professionals have been hired or contracted to work with students in-school, and over 27,000 students have been referred to some type of mental health support program since 2021.
I wonder how many of those new hires are actually licensed by a regulatory board.
And finally, Michigan has provided increased funding in recent years, including nearly $80 million in 2023 for in-school mental health services. Over half a million students attend schools with at least one provider supported by this funding.
Enough headlines. You get the idea.
Of course, there are children and teens in our nation’s schools who genuinely need mental health intervention, and K12 schools can and often do successfully identify at-risk children & youth. In partnership with other agencies and to the degree that they are able, public schools can assess these kids’ needs and get them aid.
But schools are targeting ALL the kids now. In exercising “preventative” mental health practices which are “universally applied,” schools are telling healthy youth they are sick, and they are making kids sick with the “cure.”
As author Abigail Shrier says, school-based mental health has “gone airborne.” In the name of prevention, schools target whole school populations rather than only providing help for children who demonstrate a need.
The result? More kids are reporting mental health issues than ever before:
“If people are repeatedly told that mental health problems are common and that they might experience them – and this is especially true for young people who frequently receive mental health information in schools – then it makes sense that they might start to interpret any negative thoughts and feelings through this lens.”
WHY ARE SCHOOLS DOING THIS?
It’s obvious why.
The frenzied movement to inject mental health awareness into every aspect of the school day distracts from the fact that schools are failing to educate kids. (About 40% of kids today are categorized as nonreaders, and at age 15 a mere 14% show proficiency in reading, while nearly 20% fail to meet ANY basic standards.)
Given the fact that schools’ reason for existing is to educate kids, it’s downright criminal that schools get away with filling valuable instruction time with lessons like the one pictured below, rather than focusing on facilitating student aptitude in the academic fundamentals of basic literacy, writing, and computing.
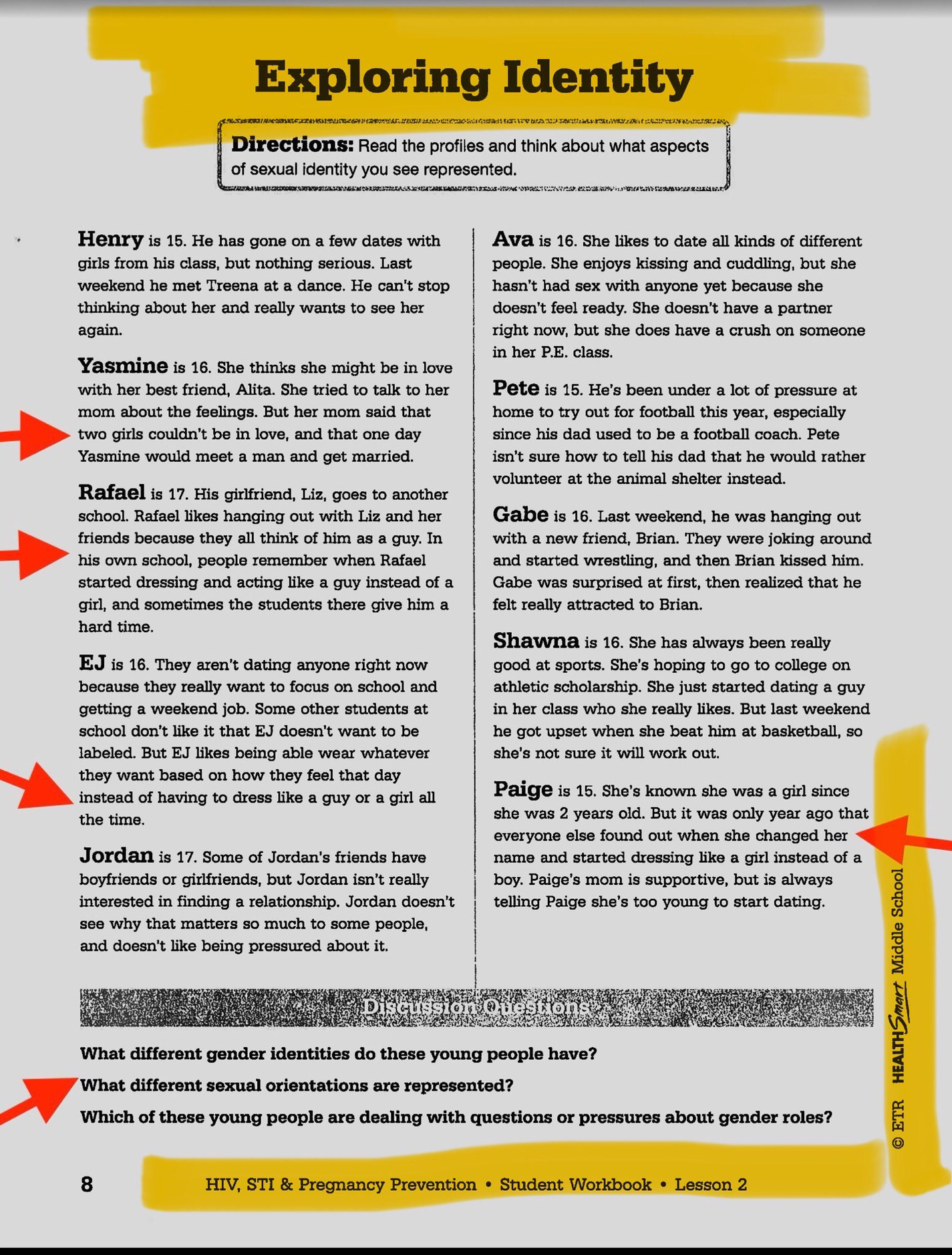
This lesson is from the HealthSmart curriculum, published by ETR, for kids aged 11 to 14 years old.
Since most U.S. students fail to show proficiency in basic academic skills, how are schools getting away with using valuable instruction time on this?
Teachers are not trained or licensed psychologists, so why do we believe it is appropriate to entrust school personnel to speak to our youth about invasive, sensitive topics like their core identities?
Should we trust school curriculum that conflates identity with sexuality to help our children build a stable sense of self?
Have we been brainwashed to think this kind of thing is OK?
The people running K12 education are convinced that schools MUST inject mental health learning into the school day, and like it or not, it’s happening. It doesn’t matter if our kids can’t read. It doesn’t matter if the research studies used to justify this sea change are unreliable. It doesn’t even matter if these interventions are shown to be ineffective and even harmful.
These efforts — with their accompanying exorbitant costs — are really not about helping kids.
Be sure to read my follow-up Stack, which defines in exacting terms the harm caused to kids by mental health curricula which 1) doesn’t know and doesn’t care what children & youth need for healthy development, and 2) operates solely to perpetuate an agenda.
#KIDSFIRST
Though this topic is complex, simply put, New Discourses James Lindsay said it well, these programs of mental health, social emotional learning, CASEL are so the kids can “take their brainwashing well.”
These programs also serve to separate child from family unit, where things that were (and should be) dealt with in family home (long term view) - the parent is excluded as the child is seen as his/her 'own unit'.